
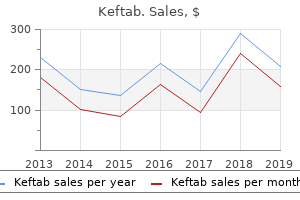
"Discount keftab line, infection zombie book".
By: X. Sven, M.A., M.D.
Clinical Director, University of Central Florida College of Medicine
Clinicians should realize that even though a symptomatic patient has a positive result on serologic testing for antibodies to B bacteria lqp-79 discount keftab line. In addition to the possibility that it is a false-positive result (a common occurrence) antibiotic quizzes purchase generic keftab on-line, the patient may have been infected with B. In addition, because symptoms never develop in some people who become infected with B. There is no indication for routine prenatal serologic screening of asymptomatic healthy women. Serosurveys have shown that the seroprevalence rates among pregnant women were comparable with those in the general population [76,77,111] and that asymptomatic seroconversion during pregnancy was unusual [76]. The difficulty arises because of the paucity of evidence that congenital Lyme disease is a clinical problem. In addition, for reasons cited earlier, the diagnosis in the mother often is inaccurate. First, parents should be reassured that there is no evidence that the infant is at increased risk of any problem from maternal Lyme disease. There is no reason to order serologic tests for Lyme disease in infants who are asymptomatic (even if diagnosis of Lyme disease in the mother is accurate). If such tests are ordered, it is important to remember that if the mother did have Lyme disease and is seropositive, the infant may have passively acquired antibodies from the mother and so may remain seropositive for many months even in the absence of infection. Because of the high frequency of false-positive test results, a positive test result for IgM antibodies against B. For patients allergic to penicillin, alternative drugs are cefuroxime axetil, erythromycin, and azithromycin. Most experts recommend a 14- to 21-day course of therapy for early localized Lyme disease, although evidence indicates that 10 days of doxycycline constitutes adequate treatment in adults with uncomplicated infection [115]. A prompt clinical response to treatment is usual, with resolution of erythema migrans within several days of initiating therapy. Occasionally, a Jarisch-Herxheimer reaction, which usually consists of an elevated temperature and worsening myalgia, develops shortly after antimicrobial treatment is initiated. These reactions typically last 1 to 2 days and do not constitute an indication to discontinue antimicrobial therapy, and symptoms respond to nonsteroidal anti-inflammatory drugs. Appropriate treatment of erythema migrans almost always prevents development of the later stages of Lyme disease. Early Disseminated and Late Disease Multiple erythema migrans and initial episodes of arthritis should be treated with orally administered antimicrobial agents. If peripheral facial nerve palsy is the only neurologic manifestation of Lyme disease, the patient can be given an oral regimen of antimicrobials. If there is pleocytosis, parenterally administered antimicrobials should Early Localized Disease Doxycycline is the drug of choice for children 8 years and older with early localized Lyme disease [112]. Exposure to the sun should be avoided by individuals who are taking doxycycline because a rash develops in sun-exposed areas 20% to 30% of the time. Preferred alternative agent for patients who cannot take either amoxicillin or doxycycline is cefuroxime axetil, 30 mg/kg/d twice daily (maximum 500 mg/dose) for 14-21 days. Erythromycin and azithromycin are less effective alternatives for patients who cannot take other recommended agents Neurologic Disease Isolated seventh cranial nerve or other cranial nerve palsy: Treat as for localized erythema migrans, but for 14-21 days (doxycycline preferred if possible) Meningitis (with or without encephalitis or radiculoneuritis): Ceftriaxone, 50-75 mg/kg once daily (maximum 2 g/dose) for 14-28 days. Alternatives include penicillin G, 200,000-400,000 U/kg/d (maximum 18-24 million U/d) every 4 hr, or cefotaxime 150 mg/kg/d (maximum 2 g/dose) divided every 8 hr for 14-28 days, and oral doxycycline, 4 mg/kg/d twice daily (maximum 200 mg/dose) for 14-21 days Carditis First-degree or second-degree heart block: Treat as for localized erythema migrans Third-degree heart block or other evidence of severe carditis: Treat as for meningitis Late Disease Arthritis Doxycycline, 2-4 mg/kg/d twice daily (maximum 100 mg/dose) for 28 days (do not use in children <8 yr old), or amoxicillin, 50 mg/kg/d twice daily (maximum 500 mg/dose) for 28 days. Preferred alternative agent for patients who cannot take either amoxicillin or doxycycline is cefuroxime axetil, 30 mg/kg/d twice daily (maximum 500 mg/dose) for 28 days. Meningitis and recurrent or persistent arthritis also should be treated with parenterally administered antimicrobial agents. Some experts prescribe a second course of an orally administered antimicrobial agent for recurrent or persistent arthritis, however, before using a parenterally administered agent. Nonsteroidal antiinflammatory drugs are a useful adjunct to antimicrobial therapy for patients with arthritis.
Rheumatoid factor may also be transiently positive antibiotics safe during pregnancy generic keftab 125mg overnight delivery, leading to some diagnostic confusion with rheumatoid arthritis in adult patients [150] most common antibiotics for sinus infection cheap 250 mg keftab free shipping. There is no joint destruction, and in most patients joint symptoms resolve within 2 to 4 weeks. For some patients, joint discomfort may last for months or, in rare individuals, years. The arthritis associated with B19 infection may persist long enough to satisfy clinical diagnostic criteria for rheumatoid arthritis or juvenile rheumatoid arthritis [89,97,149,151,152]. This finding has led some authors to suggest that B19 may be the etiologic agent of these conditions [5]. A review of the accumulated evidence on this topic has concluded that B19 is unlikely to be a primary etiology in these rheumatic diseases, but it may be one of several viral triggers capable of initiating joint disease in genetically predisposed individiuals [158]. Chronic infections may even occur in patients with more subtle defects in immunoglobulin production, who are able to produce measurable antibodies to B19, but are unable to generate adequate neutralizing antibodies [164]. B19 has also been linked to viral-associated hemophagocytic syndrome [159,160], more generally referred to as infection-associated hemophagocytic syndrome. This condition of histiocytic infiltration of bone marrow and associated cytopenias usually occurs in immunocompromised patients. B19 is only one of several viruses that have been implicated as causing viral-associated hemophagocytic syndrome. Infection-associated hemophagocytic syndrome is generally considered to be a nonspecific response to various viral and bacterial insults, rather than a specific manifestation of a single pathogen. Infections in immunocompromised hosts can lead to chronic infection; this is most often manifested as chronic anemia (red blood cell aplasia), but varying degrees of cytopenia have been described, ranging from thrombocytopenia or neutropenia to complete bone marrow failure [144]. Although most such infections are manifested as the typical persistent anemia, an association of B19 viremia with acute graft rejection has been described [168]. Data from skin biopsy of rashes temporally associated with B19 infection are limited, although several reports have been published. Only 3 of 27 children had detectable B19 IgM antibodies indicating a recent infection. The distal erythema is usually followed by petechiae or papules or purpura, and oral lesions often develop as well. A search for serologic evidence of viral infection led to the discovery of an association with acute parvovirus B19 infection in many of these patients, based on demonstration of specific IgM or seroconversion. Initially described in adults, numerous children have now been described with this condition [177]. Cases of meningitis [178,179], encephalitis [180], and encephalopathy [181] secondary to B19 infection all have been reported. Most of these are petechial or purpuric in nature, often with evidence of vasculitis in descriptions of eruptions that report skin biopsy results, and may resemble the rash of other connective tissue diseases [4,169]. Chronic B19 infection has also been associated with a necrotizing vasculitis, including cases of polyarteritis nodosa and Wegener granulomatosis [171]. These patients had no underlying hematologic disorder and were generally not anemic at diagnosis. The pathogenesis is unknown, but could suggest an endothelial cell infection as occurs with some other viruses such as rubella. At least two cases of neonatal stroke have been reported in association with B19 infection: one related to maternal infection during gestation and the other associated with infection of the newborn infant [343,344]. Disorders of the peripheral nervous system have also been described, including brachial plexus neuropathy [185], carpal tunnel syndrome [188], extremity paresthesias and dysesthesias [186], and myasthenia-like weakness [187]. The onset of most of these peripheral nerve symptoms has been coincident with the onset of rash or joint pain or both at a time when the patient should have a brisk immune response, suggesting that the neurologic abnormalities could be immunologically mediated [5]. B19 infection has also been associated with acute dilated cardiopathy, but the etiologic significance of B19 in the myocardium is unclear [201].
No test has the ability to identify all infected infants antibiotic resistance news article buy keftab mastercard, with decisions on further investigation and empirical antimicrobial therapy still requiring clinical judgment medicine for uti boots discount keftab 375mg visa. Infections of the gastrointestinal tract can be caused by one of the enterotoxins produced by S. As with all neonatal bacterial infections, cultures of appropriate samples, based on signs and symptoms of infection, physical examination, and imaging, should provide the necessary information regarding the identity and susceptibility pattern of the pathogen. The choice of empirical therapy, before susceptibility test results are known, depends on the local antibiotic resistance patterns for coagulase-positive and coagulase-negative staphylococci, the severity of infection, and the toxicity profile of the antibiotic for that infant. Culture and susceptibility information has a direct impact on selection of definitive therapy, allowing the use of the most narrowspectrum, least toxic antimicrobial regimens. Extrapolation from other pediatric and adult data is necessary, with cautions for the neonate on outcomes at dosages suggested and on the safety of these antimicrobials. For mild to moderate invasive staphylococcal infections in neonates in areas of the world where methicillin resistance is still minimal, empirical therapy with firstgeneration cephalosporins (parenteral cefazolin, oral cephalexin) or antistaphylococcal penicillins (parenteral methicillin, oxacillin, or nafcillin) is preferred. In some cases of mild skin infection, topical antibiotic therapy with mupirocin may suffice. If clindamycin is used, caution should be exercised in treating erythromycin-resistant, clindamycinsusceptible strains of S. The role of oral therapy for neonatal staphylococcal infections is not yet well defined. Trimethoprimsulfamethoxazole may be considered for mild infections in infants who no longer exhibit physiologic jaundice. Complete resistance to vancomycin is relatively recent and quite limited, with the first cases of complete resistance having been reported in 2002. By contrast, complete vancomycin resistance is still exceedingly rare and created by a different mechanism that parallels vancomycin resistance in enterococci. An initial loading dose of 15 mg/kg is most often recommended, followed by repeated dosing every 8 to 24 hours, reflecting longer dosing intervals for the youngest, most premature infants. Close monitoring of renal function and serum concentrations of vancomycin are recommended in all neonates receiving therapy, allowing for adjustment of vancomycin dosing regardless of the initial empirical dosing regimen chosen. Erythromycin is associated with the occurrence of pyloric stenosis in the newborn infant, a side effect that is likely to be less prevalent in clarithromycin and azithromycin. Clindamycin, erythromycin, and azithromycin are available in oral and intravenous formulations, but little prospective, comparative data exist for their use in neonates. Linezolid is an oxazolidinone-class protein synthesis inhibitor, the first of this new class of antibiotics. Linezolid is a ribosome-inhibiting, bacteriostatic agent, active against coagulase-positive and coagulase-negative staphylococci. Linezolid can be administered intravenously and orally, with virtually 100% of the agent absorbed by the oral route. Protein binding in plasma is approximately 30%, and the drug is well distributed into tissues. Linezolid is cleared by the kidneys, unchanged and after oxidation of the parent compound. Because oxidation of linezolid does not depend on renal function, no dose reduction is needed for renal insufficiency. Linezolid has been studied in neonates and older children for nosocomial and community-acquired pneumonia and for complicated and uncomplicated skin and skin structure infections [306,307]. The clinical response rates for each of these tissue-specific infections were equivalent to comparator agents, usually vancomycin.
Although it has not been shown antibiotics for canine ear infection keftab 500 mg on-line, it is hypothesized that cellular immunity at the mucosal level may play a role in protection against clinical varicella antibiotic resistance review cheap 500mg keftab with mastercard. Sometimes, clinical manifestations of zoster such as pain may occur in the absence of a rash-so-called zoster sine herpete. It is possible to provide humoral immunity to persons at high risk for developing severe varicella by passive immunization. Although used successfully to prevent severe varicella, passive immunization has not prevented zoster in persons at high risk for it [349], and it is not believed to be useful to treat patients with varicella or zoster [350]. Passive immunization should not be employed to try to prevent development of varicella pneumonia in the pregnant woman with chickenpox or dissemination in an already infected infant. It is uncertain whether passive immunization of a woman with varicella can prevent infection of her fetus or development of congenital varicella syndrome. Results of a large, double-blind, controlled study in healthy vaccinees older than 60 years indicated that approximately half of more than 15,000 vaccinated individuals were protected from developing zoster [354]. This study by Oxman and colleagues also indicated that there are currently about 1 million annual cases of zoster in the United States. Passive immunization has also been studied for its possible efficacy in modifying severe congenital varicella that may occur in the infant of a woman who develops chickenpox close to term. Infants born to women with the onset of varicella more than 5 days before delivery can be expected to have mild infection [62,133,289,360,361], and these infants do not require passive immunization. In contrast, infants born to women who develop varicella 5 days or less before delivery are at risk for developing disseminated or fatal varicella, and these infants can be expected to benefit from passive immunization. In an uncontrolled study by Hanngren and coworkers [290] of 41 neonates born to women who developed varicella between 4 days before and 2 days after delivery, the illness seemed to be modified. Although the attack rate was 51%, and the incubation period averaged 11 days, there were no fatalities instead of the expected mortality rate of about 30%, and 13 (62%) of 21 had fewer than 20 vesicles with no fever. The illness also seemed to be modified because of 53 infants with varicella, 74% had less than 50 vesicles, and only 10% had more than 100 vesicles. No antiviral therapy was given; there was one death in the group, but it was unclear that it was caused by varicella. The high attack rates of varicella in these studies compared with historical data have not been explained. In previous studies, infant attack rates of 24% in late [289] and overall [208] pregnancy have been reported. Successful passive immunization would, if anything, be expected to decrease the attack rate, rather than increase it. Early delivery of the infant of a mother with active varicella is also not recommended; the longer the infant remains in utero, the more likely there will be transplacental transfer of maternal antibody. The reason for the severity of these cases is not fully understood, but they seem to be unusual or rare. Passively immunized infants should be observed carefully, however, for the rare instance in which antiviral therapy may also be required. Rapid evolution of large numbers of vesicles, hemorrhagic manifestations, and respiratory involvement are indications for the use of intravenous acyclovir. Some investigators have recommended prophylactic use of intravenously administered acyclovir in any infant who develops varicella despite passive immunization [365,366,370,371], but this strategy has not been formally studied. Based on the studies cited previously, most passively immunized infants who develop clinical illness have mild or moderate infections. Administration of intravenous acyclovir to all such infants who develop clinical illness would result in needless hospitalization of many infants and potential iatrogenic problems and would not be cost-effective. Unless additional data become available, intravenous acyclovir should be given only to infants who manifest early signs of potentially severe varicella. Infants who develop varicella despite passive immunization may be given a trial of orally administered acyclovir and observed carefully for the remote possibility of development of severe varicella, at which point intravenous acyclovir may be given.
Best buy for keftab. Antimicrobial resistance is a global threat..