
"Purchase cefuroxime 250 mg free shipping, symptoms 8-10 dpo".
By: N. Varek, M.A.S., M.D.
Vice Chair, University of Texas at Tyler
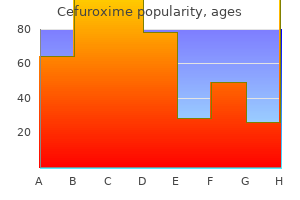
Fine-needle aspiration biopsy medications j-tube generic cefuroxime 250 mg on-line, open surgical biopsy medicine expiration dates buy cefuroxime 500 mg online, or peripheral nerve biopsy can often establish the diagnosis. The patient received a total dose of 5,600 cGy delivered by fractionated intensity modulated radiation therapy. At his 6-month follow-up, the neuroophthalmic examination was essentially unchanged. Perineural spread by squamous carcinomas of the head and neck: a morphological study using antiaxonal and antimyelin monoclonal antibodies. New-onset facial paralysis and undiagnosed recurrence of cutaneous malignancy: evaluation and management. With-out spontaneous improvement after 10 months of using prisms, he desired an alternative to prism correction. What features of the examination will help determine the cause of vertical diplopia Sashank Prasad, Department of Neurology, Division of Neuroophthalmology, Hospital of the University of Pennsylvania, 3 Gates Bldg. First, it should be established whether double vision is monocular (persists with the fellow eye closed) or binocular (abates with one eye closed). Binocular diplopia results when misaligned eyes relay contradictory visuospatial information; it therefore does not occur when viewing through one eye only. Examination should include observation of abnormal posture, such as a head tilt or head turn that the patient may use to minimize symptoms; these may also be evident on old photographs. Ocular ductions (movements of each eye individually) and versions (movements of the eyes together) should be carefully examined in all directions, to identify abnormalities of muscle weakness or overaction. Muscle overaction in a direction of gaze often signifies compensation for a long-standing or congenital process. The possibility of mechanical restriction (for example, from an orbital mass or extraocular muscle fibrosis) may be tested by evaluating forced ductions, using a cotton-tipped applicator or ophthalmic forceps to rotate the globe after applying topical anesthesia. In patients with nonrestrictive paresis, the eye can be moved the full extent of a normal duction. It is common for patients with vertical misalignment to have no visible impairment in ocular motility. In this situation, cover testing is a useful technique to identify the ocular misalignment. While the subject fixates upon a target with both eyes, the examiner covers one eye and observes for a corrective saccade in the uncovered fellow eye. This correction, termed the movement of redress, occurs if the fellow eye is misaligned and refixates. Cover testing is repeated for the second eye, and is repeated in the nine cardinal positions of gaze. In this manner, an overt misalignment of the eyes will be identified as a hypertropia (relative elevation of one eye), exotropia (relative outward position of one eye), or esotropia (relative inward position of one eye). Variations of cover testing are the cover-uncover test and the alternate cover test, in which the movement of redress is observed in the eye under cover at the time the cover is removed. The period of monocular cover causes disruption of binocular vision, allowing a latent deviation (phoria) of the eyes to be detected. Detecting a latent deviation is critical because decompensation (for example, during periods of fatigue) is a common cause of intermittent binocular diplopia. To quantify a tropia or phoria in each direction of gaze, the methods of cover testing can be performed with prism held before one eye. The Parks-Bielschowsky three-step test allows identification of the paretic cyclovertical muscle in patients with vertical misalignment. First, the hypertropic eye is identified; the paretic muscle must therefore be a depressor of one eye (inferior rectus or superior oblique) or an elevator of the other eye (superior rectus or inferior oblique). Second, it should be identified whether the hypertropia is worse in lateral gaze; hypertropia worse in contralateral gaze narrows the possibilities to weakness of the ipsilateral superior oblique or contralateral inferior rectus. Neurology 72 May 12, 2009 165 Figure 1 Eye movements and Maddox rod testing (A) Ocular motility. Note very small right hypertropia in primary gaze and upgaze, increased in left gaze. Third, it should be identified if the hypertropia is worse with head tilt; hypertropia worse with ipsilateral head tilt must be due to weakness of either the ipsilateral intorter (superior oblique) or the contralateral extorter (inferior oblique).
If the patient cannot maintain a fasting blood sugar < 95 mg/dL or a 2-hour postprandial glucose < 120 mg/dL symptoms kidney infection proven cefuroxime 250mg, then pharmacologic therapy should be considered symptoms 0f heart attack cheap cefuroxime generic. Antepartum surveillance should be initiated for pregnancies at increased risk for uteroplacental insufficiency. Table 2 shows common indications for surveillance with nonstress testing and amniotic fluid index, the corresponding gestational ages at which to initiate testing, and the recommended frequency of testing. If the culture is negative and the patient has not delivered within 5 weeks of the initial sample, obtain another sample. Recommendations for preconception, antepartum, or postpartum vaccinations include the following. Non-immune women should be vaccinated with two doses of varicella vaccine before conception, receiving the last dose at least 1 month prior to conception, or they should avoid exposure and be vaccinated in the immediate postpartum period. Nonimmune postpartum women should receive the first dose of vaccine before discharge from the health-care facility. Influenza vaccination is recommended for all women who will be pregnant during influenza season, and may be administered at any gestational age. In some studies, maternal influenza vaccination has shown benefits for the child, including a decreased incidence of fetal demise and a decreased likelihood of infant hospitalization for influenza within the first 6 months of life. For maternal antibody formation to peak around the normal time of delivery, the optimal time for administration may be around 32 weeks. Folate supplementation before and during pregnancy has been shown to reduce the risk for neural tube defects and is recommended for all patients. Folate supplementation at a dose of 1 mg daily is recommended, beginning at least three months prior to conception and continuing through the first trimester. Women with a prior pregnancy complicated by a neural tube defect should supplement their diets with folate 4 mg daily, beginning at least one month prior to conception and continuing through the first trimester. Calcium supplementation is recommended for women who have a low intake of calcium rich foods. The routine use of prenatal multivitamins is not recommended as they have not been shown to 13 improve pregnancy outcome, although they offer a convenient source of folic acid, with most formulations containing 0. Fish provides an excellent source of omega-3 oils, but should be consumed in moderation, avoiding fish high in mercury and other contaminants. Excessive weight gain during pregnancy increases the risk for complications of delivery from fetal macrosomia, such as labor dystocia, shoulder dystocia, and need for operative delivery. It also increases the risks of maternal gestational diabetes and postpartum obesity. Inadequate weight gain is associated with preterm delivery, intrauterine growth restriction, and low birth weight. Begin breastfeeding education for all pregnant women during the initial visit with the clinician. Continuing education throughout pregnancy should be offered to pregnant women who express a desire to breastfeed and for those who are still undecided on feeding method. Breastfeeding provides substantial health benefits for children (decreased ear, respiratory and gastrointestinal infections) and their mothers (decreased ovarian and breast cancer). Feeding infants artificial milk (formula) is associated with an increased likelihood of chronic disease in children (obesity, asthma and diabetes). There is no evidence of risk to fetal well-being or that prolonged activity incurs a higher risk for either pre-term labor or pre-term delivery. Regular (3 or more times weekly) mild to moderate exercise is recommended for all healthy pregnant women. The choice and amount of exercise can be tailored to the patient based on their pre-pregnancy activities. Fetal movement is a marker for fetal well-being, so counseling women to assess fetal movement can be potentially beneficial.
Regional Institute of Public Health medications while pregnant buy discount cefuroxime 500mg, Ostrava treatment 11mm kidney stone order cheap cefuroxime, Czech Republic In this report we describe a case of typhoid fever in a Czech patient with history of travel to India and discuss antibiotic treatment failure which led to the relapse of fever. Case report Travel history A previously healthy 31-year-old man from the Czech Republic visited India from 2 October to 28 November 2008. Before leaving the Czech Republic he had received neither vaccination (travellers to India are advised to get vaccinated at least against viral hepatitis A and typhoid fever) nor antimalaric chemoprophylaxis. He climbed the Himalayas, and in the last week of his stay he visited Varanasi at the Ganga River. There, he drunk a soft drink from a cup washed in water of unsure origin at the market place. His travelling companion had the same food without this soft drink, and had no problems afterwards. On 1 December the patient was examined by his general practitioner and sent to the Department of infectious diseases in Ostrava because of malaria suspicion. First hospitalisation After admission malaria was excluded, and hepatosplenomegaly was proved by ultrasonography. As fever continued, after five days of cefotaxime, ciprofloxacin of 800 mg per day was added. Cefotaxime was administered for a total of 19 days, ciprofloxacin for a total of 15 days. The patient was discharged on 22 December 2008 after 21 days of hospitalisation and after seven days without fever. Second hospitalisation At home the patient was feeling weak but his condition was gradually improving. On 31 December (nine days after leaving hospital), the patient had a new episode of fever (temperature 38. Laboratory analyses showed increasing C-reactive protein (from 42 mg/l to 96 mg/l) and decreasing platelet count (from 195 to 83 x 109/l). Finally his temperature dropped within 36 hours and the patient started to feel better without further complications. According to the World Health Organization the casefatality rates were 10-20% during the pre-antibiotic era, and can be reduced to less than 1%, with prompt and appropriate antibiotics therapy [1]. The third generation cephalosporins are now being increasingly used but they are associated with a long time of defervescence and high rates of relapses [2]. There are reports of the emergence of fluoroquinoloneresistant isolates in various part of Asia and descriptions of resistance to third-generation cephalosporins in the same region. In the case described in this paper, sensitivity tests performed during the first hospitalisation showed that S. In our patient typhoid fever therapy with ciprofloxacin plus cefotaxime showed to be ineffective, despite of adequate dose, duration of therapy and susceptibility to cefotaxime in vitro. Even though the results of blood tests were improving, the temperature declined very slowly and a relapse of typhoid fever appeared two weeks after stopping the treatment. In typhoid fever diagnostics Widal test is very commonly used but has very variable sensitivity and specificity and problems in interpretation [2]. Conclusion the 2003 World Health Organization guidelines recommend treatment with fluoroquinolones for both complicated and uncomplicated cases of typhoid fever. The third generation cephalosporins represent treatment alternative, although resistance to these drugs is gradually increasing [3]. Chloramphenicol can be an option of antibiotic choice for typhoid fever treatment when another therapy fails. Enteric fever in Mumbai-clinical profile, sensitivity patterns and response to antimicrobials. A study of typhoid fever in five Asian countries: disease burden and implications for controls.
For example medicine journey order 250 mg cefuroxime overnight delivery, a study of women in low-income housing developments found that those with a history of sexual coercion were likely to perceive that requesting a partner to use a condom would create a potentially violent situation (267) symptoms magnesium deficiency purchase cefuroxime uk. In children, the occurrence of sexually transmitted diseases can be the first indication of sexual abuse. There is also an ongoing need to determine whether new psychiatric symptoms have a medical basis that requires intervention. Title I grants provide funds to cities for low-income or under- or uninsured persons to cover the cost of health care and medications, as well as support services like counseling and home and hospice care. Psychiatric patients with common medical problems, especially those with severe mental illness, receive suboptimal medical care and suffer greater morbidity and mortality from medical illnesses than the general population. Psychiatric disorders can be underdetected, misdiagnosed, undertreated, or treated improperly in primary care settings. Underscoring the importance of mental health care is the finding that ongoing high-risk sexual behavior is predicted by higher levels of depression and recreational drug use (274). These model programs increase the opportunities for prevention and treatment and may reach a more impaired population (276). Cytochrome P450 Inhibition Potency of Protease Inhibitors, by Isoenzyme System Protease Inhibitor Cytochrome P450 Isoenzyme Inhibited Ritonavir Indinavir Nelfinavir Saquinavir 3A4, 2C9, 2D6 3A4 3A4, 2C19, 2D6 3A4, 2C9 is becoming increasingly important as a comorbid condition. Potential drug-drug interactions in the setting of antiretroviral therapy include the effects of antiretroviral agents on psychotropic medications and vice versa. Protease inhibitors and nonnucleoside reverse transcriptase inhibitors are metabolized by the cytochrome P450 system and may inhibit or induce multiple isoenzymes. For example, the protease inhibitor ritonavir inhibits the cytochrome P450 isoenzymes 3A, 2D6, and 2C9/19; thus, most psychotropic medications may be affected when concomitantly used with ritonavir. Other protease inhibitors tend to only inhibit the cytochrome P450 isoenzyme 3A, thus limiting possible drug-drug interactions to psychotropic medications metabolized via this pathway. The nonnucleoside reverse transcriptase inhibitors also require careful attention. For example, nevirapine and efavirenz are metabolized via the cytochrome P450 isoenzymes 3A and 2B6 and induce cytochrome P450 activity, which could result in decreased psychotropic concentrations at standard doses (278). Delavirdine, another nonnucleoside reverse transcriptase inhibitor, inhibits the cytochrome P450 isoenzyme 3A and reduces hepatic clearance of psychotropic agents primarily metabolized by this pathway (279). The protease inhibitors and nonnucleoside reverse transcriptase inhibitors are among the most problematic of the antiretrovirals when coadministered with psychotropic medication. Table 15 indicates the relative rank order of inhibition potency of the currently available protease inhibitors. For combination antiretroviral therapy that includes protease inhibitors and nonnucleoside reverse transcriptase inhibitors, an overarching concern in terms of coadministration with psychotropic agents is not only the possibility of plasma levels of psychotropic medications outside the targeted therapeutic concentration range but also the possible reduction of antiretroviral levels to the point of risking their effectiveness. Although the aforementioned risks for drug-drug interactions may seem substantial, to date, clinical data have not revealed severe side effects among most patients receiving antiretrovirals in conjunction with psychotropic medications (50). For example, when coadministered with ritonavir, desipramine levels have been shown to increase 145% in vitro (280) and to increase to some extent when coadministered with other protease inhibitors (281). In a clinical setting, coadministration of saquinavir and midazolam has caused prolonged sedation (282). These in vitro and in vivo data should lead to careful monitoring for potentially problematic or dangerous side effects in patients taking antiretrovirals. Other drugs of abuse, particularly those metabolized via the cytochrome P450 isoenzymes 2D6 or 3A. Although some drug-drug interactions may be only theoretical, it is prudent for clinicians to explain these concerns during the informed consent process of psychotropic prescribing. Web sites are available to clinicians and patients that address antiretroviral drug interactions and may be useful educational and reference tools ( The rational choice of psychotropic medications must also include critical considerations of adherence. Generally, it is important to minimize the number of drug doses and to tie dosing to times of the day with natural cues. However, clinicians must be cautioned that two factors may limit the generalizability of some antidepressant studies. There is, to date, no evidence to suggest adverse effects of antidepressants on the immune system (293). Nefazodone administration may theoretically decrease the metabolism of some protease inhibitors, leading to increased protease inhibitor plasma levels and increased side effects.
Cheap cefuroxime line. Robert Parker- Early Symptoms [Full EP].