
"Order mildronate 250 mg overnight delivery, medications available in mexico".
By: T. Akascha, M.A., M.D., M.P.H.
Clinical Director, University of Oklahoma College of Medicine
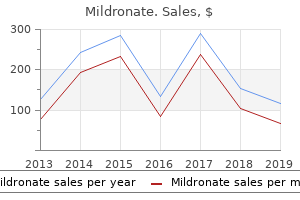
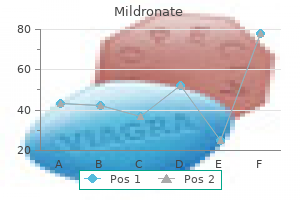
Muscle relaxant drugs together with tracheostomy or nasotracheal intubation and mechanically-assisted respiration may be lifesaving symptoms 8 days after ovulation purchase generic mildronate on-line. Signs or symptoms Incubation Infectiousness Lab specimens Prophylaxis Disease control Incubation 3-21d (perhaps 1d to several months treatment hyperthyroidism discount mildronate 250 mg without a prescription, depending on the injury) For minor wounds, immunize if <10y since last immunization. Local tetanus: Persistent contractions in same area as injury; lasts several weeks. Neonatal tetanus can result from infection at the umbilical stump if the mother is not immune. It is strongly recommended to study the scientific publications and textbooks related to a certain topic. Myoelectric signals are formed by physiological variations in the state of muscle fiber membranes. The term units outlines the behavior, that all muscle fibers of a given motor unit act "as one" within the innervation process. Muscle Fibers Axon Motor endplates Motor Unit Alpha Motoneuron Excitation Excitation Excitability of muscle membranes. Adopted & modified from 2,7 the excitability of muscle fibers through neural control represents a major factor in muscle physiology. This phenomenon can be explained by a model of a semi-permeable membrane describing the electrical properties of the sarcolemna. An ionic equilibrium between the inner and outer spaces of a muscle cell forms a resting potential at the muscle fiber membrane (approximately -80 to -90 mV when not contracted). This difference in potential which is maintained by physiological processes (ion pump) results in a negative intracellular charge compared to the external surface. The activation of an alpha-motor anterior horn cell (induced by the central nervous system or reflex) results in the conduction of the excitation along the motor nerve. After the release of transmitter substances at the motor endplates, an endplate potential is formed at the muscle fiber innervated by this motor unit. The diffusion characteristics of the muscle fiber membrane are briefly modified and Na+ ions flow in. It is a monopolar electrical burst that is immediately restored by the repolarization phase and followed by an After Hyperpolarization period of the membrane. Starting from the motor end plates, the action potential spreads along the muscle fiber in both directions and inside the muscle fiber through a tubular system. Linked chemical processes (Electro-mechanical coupling) finally produce a shortening of the contractile elements of the muscle cell. This model linking excitation and contraction represents a highly correlated relationship (although weak excitations can exist that do not result in contraction). From a practical point of view, one can assume that in a healthy muscle any form of muscle contraction is accompanied by the described mechanisms. After initial excitation this zone travels along the muscle fiber at a velocity of 2-6m/s and passes the electrode side: Differential Amplifier Skin Electrodes Display Unit Sarkolemm -+++ +++ - Depolarized membrane area Front of excitation Direction of propagation. For simplicity, in a first step, only the detection of a single muscle fiber is illustrated in the following scheme. Depending on the spatial distance between electrodes 1 and 2 the dipole forms a potential difference between the electrodes. In the example illustrated in figure 9, at time point T1 the action potential is generated and travels towards the electrode pair. An increasing potential difference is measured between the electrodes which is highest at position Depolarisation wave Differential Amplifier Electrodes Display Unit + T1 + T2 + T3 + T4 + T5 T2. If the dipole reaches an equal distance between the electrodes the potential difference passes the zero line and becomes highest at position T4, which means the shortest distance to electrode 2. This model explains why the monopolar action potential creates a bipolar signal within the differential amplification process. Because a motor unit consists of many muscle fibers, the electrode pair "sees" the magnitude of all innervated fibers within this motor unit - depending on their spatial distance and resolution. Because the human connective tissue and skin layers have a low pass filter effect on the original signal, the analyzed firing frequency. Assuming a state-of-the-art amplifier performance and proper skin preparation (see the following chapters), the averaged baseline noise should not be higher than 3 5 microvolts, 1 to 2 should be the target. Be careful not to interpret interfering noise or problems within the detection apparatus as "increased" base activity or muscle (hyper-) tonus! This is due to the fact that the actual set of recruited motor units constantly changes within the matrix/diameter of available motor units: If occasionally two or more motor units fire at the same time and they are located near the electrodes, they produce a strong superposition spike!
Examples include achondroplasia treatment lice buy generic mildronate 500 mg line, neurofibromatosis medications dialyzed out cheap mildronate 500 mg overnight delivery, Marfan syndrome, and myotonic dystrophy. Some X-linked dominant diseases are known, but for most of them, no data on incidence estimates are currently available. The general point with respect to Mendelian diseases is that the relationship between mutation and disease is simple and predictable. Multifactorial Diseases the major burden of naturally occurring genetic diseases in human populations, however, is not constituted by Mendelian diseases, which are rare, but by those that have a complex etiology. The term "multifactorial" is used to designate these diseases to emphasize the fact that there are multiple genetic and environmental determinants in their etiology. Examples of multifactorial diseases include the common congenital abnormalities such as neural tube defects, cleft lip with or without cleft palate, and congenital heart defects that are present at birth, and chronic diseases of adults. Evidence for a genetic component in their etiology comes from family and twin studies. For example, first-degree relatives of patients affected with coronary heart disease have a two- to sixfold higher risk of the disease than those of matched controls, and the concordance rates of disease for monozygotic twins are higher (but never 100%) than those for dizygotic twins (Motulsky and Brunzell 1992; Sankaranarayanan and others 1999). As mentioned earlier, multifactorial diseases are presumed to originate from the joint action of multiple genetic and environmental factors; consequently, the presence of a mutant allele is not equivalent to having the disease. For these diseases, the interrelated concepts of genetic susceptibility and risk factors are more appropriate. The genetic basis of a common multifactorial disease is the presence of a genetically susceptible individual, who may or may not develop the disease depending on the interaction with other genetic and environmental factors. The important general point is that unlike the situation with Mendelian diseases, the relationships between mutations and disease are complex in the case of multifactorial diseases. For most of them, knowledge of the genes involved, the types of mutational alterations, and the nature of environmental factors remains limited. As discussed later, this is really not an etiological category, and deletions (microscopically detectable or not) are now known to contribute to a number of constitutional genetic diseases grouped under autosomal dominant, autosomal recessive, and X-linked diseases. One such indirect method is the doubling dose method, on which attention is focused in this section. The Doubling Dose Method the doubling dose method enables expressing of the expected increase in disease frequency per unit dose of radiation in terms of the baseline frequency of the disease class. The theory assumes that the stability of mutant gene frequencies (and thus disease frequencies) in a population is the result of the existence of a balance between the rates at which spontaneous mutations enter the gene pool in every generation and the rate at which they are eliminated by natural selection. When the mutation rate is increased as a result of radiation in every generation, this balance between mutation and selection is disturbed by the influx of induced mutations, but the prediction is that the population will attain a new equilibrium (over a number of generations) between mutation and selection. The amount of increase in mutation frequency, the time it takes for the population to reach the new equilibrium, and the rate of approach to equilibrium are all dependent on induced mutation rates, the intensity of selection, the type of genetic disease, and whether the radiation exposure occurs in one generation only or generation after generation. Risk Estimation for Different Classes of Genetic Disease the application of Equation (4-2) to risk estimation is straightforward for autosomal dominant diseases since the relationship between mutation and disease is simple for this class of diseases. Population genetic theory predicts that for these diseases, if there is an x% increase in mutation rate in every generation, at the new equilibrium this increase will be reflected as an x% increase in the frequency of these diseases. Until recently, estimates of risk for the first, second, or any postradiation generation of interest were obtained through "back calculation" from the predicted new equilibrium incidence using certain assumptions. If the population sustains radiation exposure in one generation only, there will be a transient increase in the mutant frequency in the first postradiation generation, followed by a progressive decline to the "old" equilibrium value. The method used to predict the risk of X-linked diseases is approximately similar to that for autosomal dominant diseases discussed above. For autosomal recessive diseases, the risk calculation is more involved because when recessive mutations first arise (or are induced), they are present in the heterozygous state and do not precipitate disease in children of the first few postradiation generations. The mutation component is defined as the relative increase in disease frequency. During the past few years, the concept has been developed further with the necessary algebraic formulations, that permit a direct evaluation of the impact of an increase in mutation rate for all classes of genetic disease in any postradiation generation of interest following exposure to radiation in either one generation only or generation after generation (Chakraborty and others 1998a; Denniston and others 1998). Advances in human genetics during the past two decades now permit an upward revision of the above estimates to 1. To the extent that genetic influences are important, the effects are through genes that have small individual effects but that act cumulatively among themselves and in combination with environment factors to increase susceptibility. The estimates vary over a wide range, from about 1% in live births to a high of about 8. This documents the premise that under conditions of good ascertainment, the overall prevalences are similar and are of the order of about 6%. This committee therefore accepts the 6% figure as reasonable for use in risk estimation in this report.
Order genuine mildronate line. EARLY SIGNS OF AUTISM IN 18 MONTH OLD TODDLERS.
When standing for long periods of time symptoms of kidney stones cheap 250 mg mildronate amex, shift your weight from leg to leg x medications buy mildronate master card, stretch and walk about some, or sit for a few minutes. However, these simple measures, along with the passage of time, will provide relief to the vast majority of people. If your pain is getting more severe or frequent despite these recommendations, or if you are having pain or numbness radiating down into your arms, please let the doctor know, in case further evaluation is in order. Neck and Shoulder Relaxation Exercises Do these exercises times each, times a day. With your arms bent at the elbows, push back to bring your shoulder blades together at your back. Conlosbrazosflexionadosala altura de los codos, haga fuerza hacia atrбs, para juntar los omуplatos en la espalda. With your arms straight out in front of you, reach forward stretching your arms as far as you can. The medical information found on this website should not be used in place of a consultation with your doctor or other health care provider. Con los brazos estirados hacia adelante, procure que se estiren lo mбs lejos posible. You should always seek the advice of your doctor or other qualified health care provider before you start or stop any treatment or with any questions you may have about a medical condition. Citation for this document: Royal College of Physicians, British Society of Rehabilitation Medicine, the Chartered Society of Physiotherapy, Association of Chartered Physiotherapists in Neurology and the Royal College of Occupational Therapists. No part of this publication may be reproduced in any form (including photocopying or storing it in any medium by electronic means and whether or not transiently or incidentally to some other use of this publication) without the written permission of the copyright owner. It presents in a variety of ways depending on the size, location and age of the lesion, and may have a number of harmful secondary effects such as pain, deformity and impaired function. Spasticity management is challenging due to the diversity of patient presentation and goals or aims of treatment. There is a strong body of Level I evidence for its effectiveness in the management of both upper and lower limb spasticity. The principles for successful intervention are: ° appropriate patient selection ° establishment of clear goals for treatment ° clear establishment of the immediate and ongoing treatment programme. It has also become an accepted part of routine management of spasticity in other muscle groups, such as neck and jaw muscles. It should not be used in isolation, but as part of a coordinated multidisciplinary approach, involving physical management and therapy, to achieve the desired effect. Common goal areas for intervention include: ° pain relief ° reduction of involuntary movements (eg associated reactions, spasms) ° prevention of contractures and deformity ° passive function (making it easier to care for the affected limb) ° active function (using the affected limb) ° mobility. Treatment goals should be agreed between the team and the patient and/or their family, and documented. In the last decade a substantial body of work has been undertaken to develop a consistent approach to outcome measurement that can be used internationally. The rationale for this is to combine a person-centred approach to goal setting and outcome measurement, which provides comparable information across different populations, practices and programmes of care and avoids excessive burden in data collection. Strong 2 Principles of coordinated spasticity management Grade of evidence E1 E2 Strength 2. Clinicians should refer to Appendix 2 for the recommended doses for individual muscles. Task-practice training (repetitive practice) should be considered when improvement in activity performance and motor control are the target or goal of treatment. Strong © Royal College of Physicians 2018 xi Spasticity in adults: management using botulinum toxin 6 Follow-up, documentation and outcome evaluation Grade of evidence E1 E2 Strength 6. Injections should be followed by a formal assessment of outcome that includes: · severity of presentation at baseline · achievement of intended goals for treatment using Goal Attainment Scaling · standardised measures selected according to the goals for treatment. Outcome evaluation should be standardised as far as possible to support comparison for quality benchmarking and research.
Inverse dose-rate effect for mutation induction by gamma-rays in human lymphoblasts medicine vocabulary mildronate 500 mg fast delivery. A comparison of induced mutations at homologous alleles of the tk locus in human cells symptoms west nile virus purchase mildronate 250 mg fast delivery. A locus that influences susceptibility to 1,2-dimethylhydrazine-induced colon tumors maps to the distal end of mouse chromosome 3. A two-stage theory of carcinogenesis in relation to the age distribution of human cancer. Circulating anti-Helicobacter pylori immunoglobulin A anitbodies and low serum pepsinogen I level are associated with increased risk of gastric cancer. Occupational exposure to ionising radiation and mortality among workers of the former Spanish Nuclear Energy Board. Telomere dysfunction promotes non-reciprocal translocations and epithelial cancers in mice. Prevalence of goiter and urinary iodine excretion levels in children around Chernobyl. First analysis of mortality and occupational radiation exposure based on the National Dose Registry of Canada. Investigation of an excess of melanoma among employees of the Lawrence Livermore National Laboratory. Radiation-induced adaptive response for protection against micronucleus formation and neoplastic transformation in C3H 10T1/2 mouse embryo cells. Low-dose ionizing radiation decreases the frequency of neoplastic transformation to a level below the spontaneous rate in C3H 10T1/2 cells. Intercellular communication is involved in the bystander regulation of gene expression in human cells exposed to very low fluences of alpha particles. Oxidative metabolism modulates signal transduction and micronucleus formation in bystander cells from alpha-particle-irradiated normal human fibroblast cultures. Impact of ionizing radiation and genetic background on mammary tumorigenesis in p53-deficient mice. Elevated mutation rates in the germ line of first- and second-generation offspring of irradiated male mice. Loss of the ataxia-telangiectasia gene product causes oxidative damage in target organs. Occupational exposure to radiation induces an adaptive response in human lymphocytes. Screening for putative radon-specific p53 mutation hotspot in German uranium miners. Leukemias and lymphomas in Ukraine population exposed to chronic low dose irradiation. Historical and current highlights in radiation biology: has anything important been learned by irradiating cells? A polymoprhic locus near the human insulin gene is associated with insulin-dependent diabetes mellitus. Direct evidence for a bystander effect of ionizing radiation in primary human fibroblasts. Environmental tobacco smoke, genetic susceptibility, and risk of lung cancer in never-smoking women. Cell density dependence of transformation frequencies in C3H10T1/2 cells exposed to x-rays. Evidence for pronounced bystander effects caused by nonuniform distributions of radioactivity using a novel three-dimesional tissue culture model. Statistical issues in assessing the evidence associating obstetric irradiation and childhood malignancy. Pre-natal irradiation and childhood malignancy: a review of British data from the Oxford Survey.