
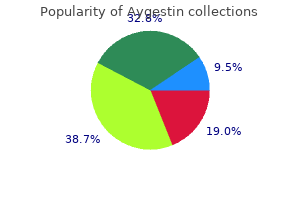
"Discount aygestin line, women's health problems and solutions".
By: U. Stan, M.A., M.D.
Professor, University of Utah School of Medicine
Results: At 7 Italian Centers menstrual interval purchase aygestin in united states online, we included 20 patients satisfying the 1st (n=1) menstruation on full moon purchase 5mg aygestin with mastercard, 2nd (n=2), or 3rd (n=17) criterion. In the control cohort, A/A genotype carriers had poor tumor response in overall (P =. In part 2, expansion cohorts including patients with thymic, pancreatic, triple-negative breast carcinoma, or solid tumors with TrkA alterations will be accrued to further evaluate safety and efficacy. First Author: Hagen P Schwenzer, University of Oxford, Oxford, United Kingdom Background: Nucleoside analogs form the backbone therapy for both hematological and solid malignancies. However, their clinical effectiveness is severely limited by key cellular resistance mechanisms linked to increased breakdown, impaired activation and transport. Methods: NuTide:701 is a two-part, first-in-human Phase I study in patients with advanced solid tumors and lymphoma who have exhausted all standard treatment options. Methods: Patients are treated with Aza-TdC on days 1-5 and 8-12 of each 21-day cycle. The study follows Simon accelerated titration design 3, with 100% dose increments and 1 patient per dose level. Patients included in this study must be $18 years old and have histologically documented solid tumors that have progressed on standard therapy and for which there is no other standard therapy available. First Author: Jade Maxime van Berge Henegouwen, Leiden University Medical Center, Department of Medical Oncology, Leiden, Netherlands Background: With the emergence of large-scale genetic tumor profiling and the increasing availability of approved targeted therapies, precision medicine has become crucial in cancer treatment. However, for many cancers the relative contribution of either tumor type or genetic aberration to drug sensitivity often remains unknown. Since drug access is generally limited to the on-label indication and outcome of off-label use is not systematically collected in clinical practice, innovative trials facilitating drug access, whilst systematically analyzing treatment outcomes, are urgently needed. All submitted patients are reviewed and enrolled in multiple parallel cohorts, preceded by a baseline tumor biopsy for whole genome sequencing to confirm previously identified variants and for exploratory biomarker analyses. Each cohort is defined by a study drug, histologic tumor type, and molecular tumor profile. Primary endpoints include objective response rate, stable disease at 16 weeks, and grade $3 adverse events. Since the start of recruitment in September 2016, 870 patients have been submitted for review and 365 patients (42%) have started treatment in one of 101 opened cohorts. Eight cohorts have graduated to the second stage, two cohorts completed accrual in either their first or second stage, and one cohort was closed due to a registered indication. In other cases, study results were disappointing, likely due to the rarity of molecular alterations, limits in trial design and the difficulties in applying molecular tumor profiling in the clinical setting. BoB is a novel platform trial from Cancer Core Europe, a recently established sustainable European network for innovative cancer research. It also enables testing/developing companion diagnostics linked with the therapeutic part (part B). Each module is focused on a certain molecular pathway or on certain molecular alterations that may confer sensitivity to the study drug or study drug combination evaluated in that module/arm. Our final aim is to achieve drug repurposing of treatments, codevelop multi-marker companion diagnostics and a large database of knowledge in Precision Medicine. Grade $3 adverse events in $5% of pts were neutropenia/neutrophil count decreased (38%), anemia (13%), hypophosphatemia (11%), diarrhea (9%), fatigue (9%), and febrile neutropenia (7%). Patients are also required to have an Eastern Cooperative Oncology Group Performance Status score of 0 or 1 and creatinine clearance $30 mL/min. Understanding prostate cancer biology with tumor biopsies does not address the issue of tumor heterogeneity or cellular degradation during the decalcification process of bone biopsies. Upon enrollment, subjects will have baseline assessments with standard cross-sectional imaging, 99mTc bone scan, and blood work. To precisely stratify breast cancers into actionable subgroups, full genome expression data and matching clinical data must be aggregated into a large data set. Such a data set will accelerate research and discovery, especially for smaller patient subsets who are not as widely represented within the current body of literature. Secondary objectives include utilizing the shared study infrastructure to examine and generate hypotheses for targeted subset analyses and/or trials based on full genome expression data. Patients enrolled in the initial study are also eligible for inclusion in sub-studies where they meet all criteria and additional consent is not required.
The subglottis begins below the level of the true vocal cords and extends to the first tracheal ring menopause 2 periods a month purchase aygestin 5 mg. The cartilaginous structures of the epiglottis menopause guidelines purchase cheap aygestin on-line, thyroid cartilage, arytenoid cartilage, and cricoid cartilage can be easily distinguishable on imaging. The cricoid cartilage is the only intact ring of the larynx, having a complete posterior component. The inferior margin of the arytenoid cartilage with its vocal process marks the border of the true vocal cord. This coronal T1-weighted scan shows the separation of the supraglottis from the glottis by the laryngeal ventricle (short arrow). Note that the paraglottic tissue at the level of the false vocal cords and above is highintensity fat (long arrow). The paraglottic tissues can be separated into the pre-epiglottic fat, the paraglottic fat, and the thyroarytenoid muscle of the true vocal cord. The differentiation between preepiglottic fat and paraglottic fat is important from the standpoint of some of the T-staging issues that require addressing the preepiglottic fat [10]. Nonetheless, the thin septum that separates paraglottic from preepiglottic fat is often invisible on imaging studies, and therefore the border zone between these two tissues can be blurred. The significance of preepiglottic fat invasion lies in the potential need to address the base of the tongue in surgical resection and the danger to the hyoid bone, which is required in the supracricoid surgeries. While this is best assessed endoscopically, the imaging correlates to tumoral fixation are cricoarytenoid joint involvement, interarytenoid disease, and paraglottic spread [15]. Because transglottic extension is critical to the differentiation between supraglottic laryngectomy surgery for supraglottic carcinomas and vertical hemilaryngectomy surgeries for glottic carcinomas, coronal reconstructions and/or direct coronal scanning is highly recommended as part of the laryngeal imaging protocol with any modality. Often, the spread is not along the mucosa (where it is evident to the endoscopist) but is in the paraglottic space and/or submucosal space where the disease may be invisible, even to the trained eye [16]. For the radiologist, the source of the tumor (whether from a glottic or supraglottic origin) may not be as obvious as at endoscopy; however, the deep spread from one compartment to the other is apparent on these imaging modalities. The strandiness is related to minor salivary gland tissue in this location, a source of falsepositive studies. Hyoid bone invasion may prohibit the supracricoid laryngectomy surgeries because the hyoid bone is needed as part of the ``pexy' procedure. Because the thyroid cartilage may be either chondrified or ossified, it is the most difficult cartilage of the larynx to evaluate for tumor erosion. The density of nonossified cartilage is similar to squamous cell carcinoma and has similar intensity on T1-weighted scans. Coronal T1-weighted scan shows a mass (T) that crosses the plane of the supraglottic and glottic larynx, extending in a paraglottic location into the thyroarytenoid muscle. Note the width of the paraglottic soft tissue on the left side compared with the right side. This lesion was seen only as a supraglottic mucosal lesion, and the extent across the plane of the laryngeal ventricle was unexpected. This supraglottic carcinoma had both a mucosal lesion and a deep submucosal mass on the left side. Note that the thyroid cartilage, which is normal, shows areas of high signal intensity on the T1-weighted scan, representing ossification (short arrows), and areas of lower signal intensity, representing chondrification (long arrows). On a fast-spin echo T2-weighted scan or T1-weighted scan with fat suppression, all of these areas would be dark. There are focal erosions and low-density areas in the midline near the thyroid notch (short white arrow). The changes were from inflammatory reactive change rather than neoplastic infiltration from the true vocal cord cancer. This was an extensive supraglottic carcinoma which spread transglotticly and posteriorly. Whereas sclerosis was the most sensitive (83%) criterion in all of the cartilages, histopathologically it often corresponded to reactive inflammation, particularly in the thyroid cartilage (specificity, 40%).
Indications for these procedures include multiple tumors teva women's health birth control guide cheap aygestin 5 mg overnight delivery, generally 4 or more in number breast cancer 2a purchase 5mg aygestin with mastercard, lesions greater than 3 to 5 cm, lesions without vascular invasion or extrahepatic spread. Absolute contraindications include decompensated cirrhosis, jaundice, clinical encephalopathy, refractory ascites, hepatorenal syndrome, extensive tumor replacement of both lobes, portal vein occlusion or severely reduced flow, hepatofugal flow and renal insufficiency. Some controversy has existed over the size of eligible lesions with initial restriction to lesions of up to 5 cm now being expanded to larger lesions. Current optimal dose recommendations are 50 Gy in 5 treatment fractions with a mean liver dose of 13. The unique dosimetric advantages of heavy charged particle radiation (Bragg Peak) offer significant potential advantages in sparing hepatic parenchyma compared to traditional photon techniques. This theoretical advantage is still the object of ongoing studies in this country. They found a 19% increase in secondary primary malignancies in seminoma patients exposed to radiation therapy as compared to the general population including pancreas, non-bladder urothelial, bladder, thyroid, and others. They identified risks of lung, bladder, pancreas, stomach, and other organs, noting that secondary primary cancers are a leading cause of death in men with a history of testicular cancer. The use of protons brings a distinct advantage in lowering radiation dosed to the population at risk. It is noted that six patients developed radiation necrosis (who all survived at least four years without evidence of recurrence, but in whom the performance status had declined by 10 to 30%). The authors, however, conclude that "The overall potential clinical benefit of these dosimetric advantages in glioblastoma patients remains to be determined. The reduction in the volume of tissue receiving low doses of radiation has not clearly been associated with improved clinical outcomes. The 3-year overall, relapse-free, distant metastasis-free, and locoregional-free survival rates were 51. It should be noted that this was not a randomized study and treatment eras as well as clinical factors were not the same for the different groups. All patients had initially non-metastatic cancer treated with neoadjuvant concurrent chemoradiotherapy and surgical resection. This especially pertains to targets in the thorax and upper abdomen, including the distal esophagus that move as a result of diaphragmatic excursion (Mori and Chen, 2008; Mori et al. Skin toxicity, fatigue and radiation pneumonitis were evaluated during radiation and at 4 and 8 weeks after completing radiation. The authors reported grade 2 and 3 acute dermatitis in 72% and 5% respectively with 21% requiring opioids for pain control and 8% requiring a treatment break. Seven patients developed a skin infection requiring antibiotics, one of which resulted in nonlethal sepsis. Another patient developed a non-healing wound requiring closure with a latissimus flap. This study will help determine the benefit of proton beam therapy in the treatment of breast cancer in patients receiving comprehensive nodal radiation. There was no statistically significant difference in gastrointestinal or other toxicity at 6 months or 12 months post-treatment. Toxicity associated with prostate radiation is more closely associated with high dose exposure of normal tissues, > 50 Gy. Proton beam therapy for primary treatment of prostate cancer should only be performed within the context of a prospective clinical trial or registry. There is no clear evidence that proton beam therapy for prostate cancer offers any clinical advantage over other forms of definitive radiation therapy. Clinical trials are necessary to establish a possible advantage of this expensive therapy. Hypo-fractionation With Proton Radiation Therapy for Low Risk Adenocarcinoma of the Prostate D. There were no significant differences between the groups with each group receiving 70 Gy.
Syndromes
- Bruise or scrapes on the chest wall
- Surgery, called carotid endarterectomy, is done to remove the buildup in your carotid arteries. See: Carotid artery surgery
- Purpura
- Feces of dogs, wolves, or coyotes
- Sharp or severe abdominal pain, especially if you also have bloating
- Cloudy or bloody urine, which may have a foul or strong odor
Pts receive 17 cycles of pembrolizumab 200 mg Q3W plus standard thoracic radiotherapy in cycles 2 and 3 (60 Gy in 30 daily 2 Gy fractions) pregnancy 0-4 weeks discount 5 mg aygestin with mastercard. Approximately 216 pts (108 per cohort) will be enrolled in 59 sites in 10 countries beginning on Nov 5 menstruation visceral fat purchase 5 mg aygestin free shipping, 2018. Continuous interim analyses using binomial sequential testing will be performed after $36 pts have $15 weeks of follow up in each cohort, to allow earlier treatment discontinuation, if required. Cell dose escalation/de-escalation decisions will be guided by a modified toxicity probability interval design. In the dose exploration phase, patients will be monitored for doselimiting toxicities during the first 28 days. A Bayesian logistic regression model will be used to inform dose escalation/de-escalation decisions. However,prophylactic cranial irradiation can lead to decline in cognitive function. Preclinical evidence suggests that the pathogenesis of this toxicity includes inflammatory injury to proliferating neuronal progenitor cells in the peri-hippocampal stem cell niches. Results: 449 pts were randomized characteristics were balanced between treatment arms: Asian 77%, Females 63%, Ex19del 54%. Safety was consistent with the established safety profiles of the individual compounds. Restaging was every 2 to 3 mths; therapy continued until progression or intolerable toxicity. Results: Between Aug 2016 and Aug 2018, 350 patients were randomly assigned to gef (n = 177) and gef+C (n = 173). Clinically relevant $ grade 3 toxicities occurred in 51% and 25% of patients in gef+C and gef arms respectively, P, 0. Conclusion: Adding pemetrexed-carboplatin chemotherapy to gefitinib significantly prolonged progression free and overall survival but also increased toxicity. The combination of bevacizumab and pemetrexed cannot be recommended due to the lack of survival benefit in this definitive study. We conducted a randomized trial of Bev versus Bev+Pem as continuation maintenance therapy after Car+Pem+Bev induction therapy. Those who showed no progression during the induction therapy were randomized to receive maintenance therapy using Bev or Bev+Pem in a 1:1 ratio. The planned sample size was 620 to provide a power of 85% at one-sided significance level of 5%. Violations found at a study site led us to conduct source document verification for 95. Results: Between September 2010 and September 2015, 907 patients had the induction therapy. Of those, 621 patients were randomized; five did not receive study treatment and 22 did not meet the eligibility criteria. First Author: Juergen Wolf, Lung Cancer Group Cologne, University of Cologne, Faculty of Medicine and University Hospital of Cologne, Dept. Acquired resistance (Jackman criteria) was seen in 29 patients, 9 with paired pre-/post-treatment samples. Results: As of 11 Nov 2018, 15 pts (6 M; 9 F) were enrolled across 3 dose levels (3. Methods: Eligible pts were randomized 2:1 to pembro (n = 410) or placebo (n = 206) + pemetrexed and carboplatin or cisplatin for 4 cycles followed by pembro or placebo for up to 35 cycles + maintenance pemetrexed. Results: From December 18, 2015 to April 23, 2018, 275 pts enrolled and 252 determined eligible (125 N+I and 127 N). Additional cutoffs and outcomes in subgroups defined by both biomarkers will be presented. Interpretation of these data may be limited by small sample sizes; further investigations are warranted.
Buy aygestin 5mg fast delivery. Practice Yoga Like Jennifer Aniston from Women's Health.